Jessica Ressel-Doeden was diagnosed with a diffuse, intrinsic, childhood brainstem glioma (DIPG) in March of 1996 at age eleven.
According to the available data there has not been a single case of a verified cure (5-year survival) with patients diagnosed with diffuse (inoperable) childhood brainstem glioma treated with radiation and/or chemotherapy in any FDA-supervised experimental clinical trial in the history of medicine. Dr. Burzynski’s Antineoplastons hold the only cures to date—with a cure rate in some studies as high as 27.5% [PDF of original report, table page 172] + [Chemo/Rad – PubMed 2005] [ANP – PubMed 2003] [ANP – PubMed 2006] [ANP – Cancer Therapy 2007]
[The Lancet 2006 explains grim outlook – “survival remains static”].
** April 2014 Peer-reviewed clinical trial report for DIPG using Antineoplastons **
Following her initial diagnosis, the Ressel’s were informed that the only method approved by the FDA to “treat” her condition would be radiation. The radiologist informed the family that radiation would be shot “through the ears, burning her healthy cells from the outside in—causing permanent deafness, all of the hair around her ears would be gone—never grow back, her ears would become deformed and burnt, her pituitary gland would be destroyed—the gland that allows a human to grow and develop, and if she survived the treatment she would become a vegetable and incapable of taking care of herself.”
Considering that radiation treatment has never been shown to cure a single patient with her condition, combined with the devastating side effects such a treatment would inflict on an eleven-year old child—her parents declined the radiation treatment offered by her oncologists and decided to have Jessica treated by Dr. Burzynski instead.
Medical Records
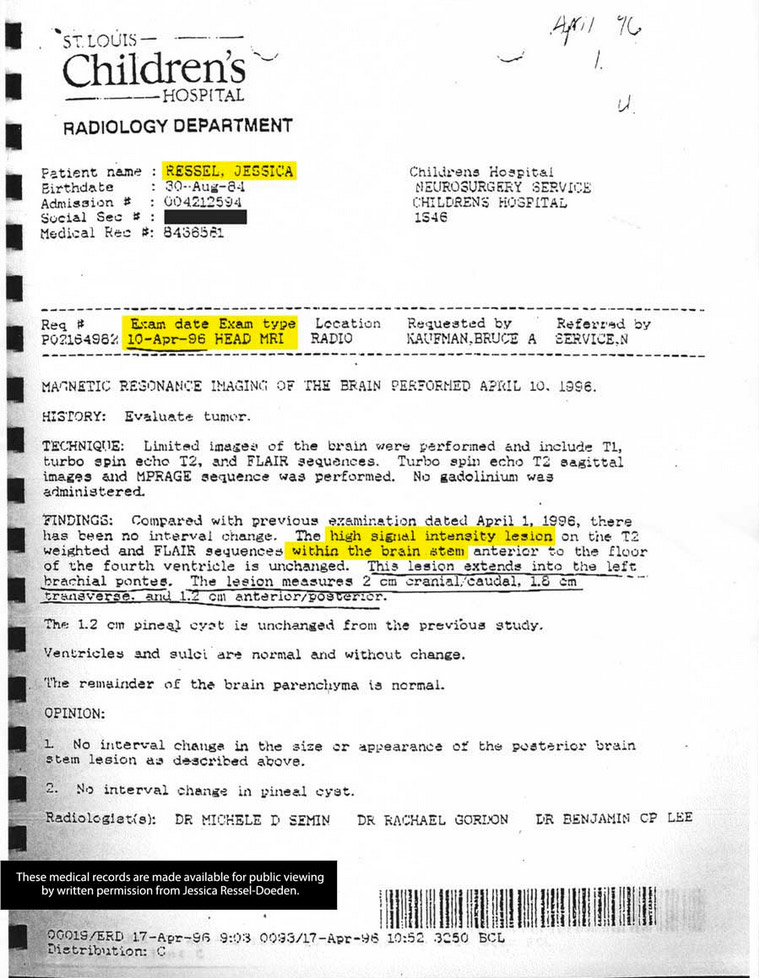
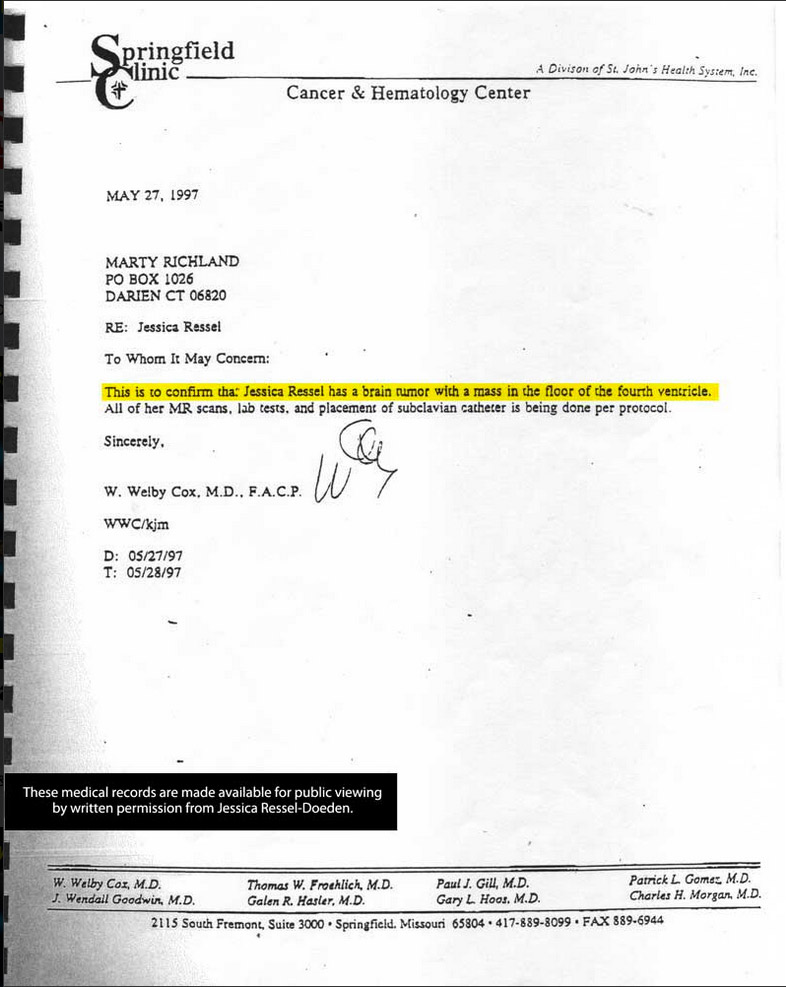
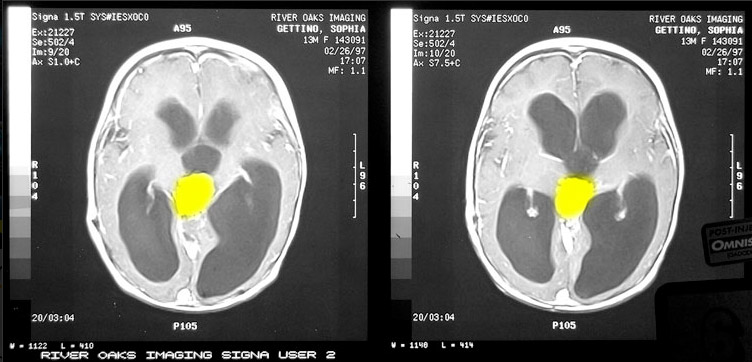
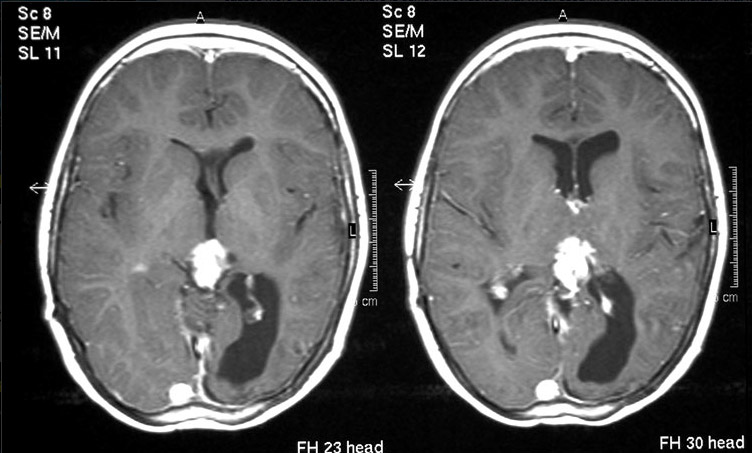
1. Diagnosis: Jessica underwent an MRI on April 10, 1996 at the St. Louis Children’s Hospital which revealed a tumor in her brainstem. Her diagnosis was also confirmed on May 7, 1996 upon initial consultation with Dr. Burzynski. She had multiple MRIs after she was admitted into the Burzynski Clinic. There is also multiple third-party confirmations of diagnosis by physicians from the Springfield Clinic and the Missouri Eye Institute demonstrated by letters written to the Ressel’s insurance company.
2. Recovery: On May 8, 1996, Jessica began antineoplaston treatment. Her tumor disappeared and reappeared multiple times throughout the course of 14 months after the start date of treatment. On June 27, 1997, her tumor disappeared permanently. She has had multiple MRIs of the brain since that time which have all been negative for tumor recurrence—with the last MRI being May 20, 2005. Read Jessica’s treatment summary here. Read Jessica’s tumor measurements here. After her full recovery, the Mid-Atlantic Open MRI of Springfield, MO confirmed her tumor-free MRIs from 11/97 to 5/98 [PDF all medical records and sources for this paragraph].
3. FDA-supervised clinical trial data comparing chemotherapy and radiation treatment to antineoplaston treatment in patients with diffuse, intrinsic, childhood brainstem glioma. It has been clearly demonstrated that of 107 patients treated with chemotherapy and radiation with this type of tumor: 0.9% of these patients were cancer-free at the end of treatment, with no patient surviving 5 years after diagnosis. Of the patients treated with antineoplastons with this type of tumor: 27.5% of them were cancer-free at the end of treatment, with 27.5% of the patients living at least 5 years after diagnosis. Therefore, Jessica Ressel’s recovery after being treated with antineoplastons is not a mere anecdotal case (See sources from start of this post above).
Most would assume that such results would be front page news across the world, or would be grounds for Dr. Burzynski to receive the Nobel Prize in medicine. Sadly, these peer-reviewed results have been universally ignored by mainstream medicine.
Raising the Money to Receive Her Antineoplaston Treatment
Unfortunately, most insurance companies will not cover antineoplaston treatment. The Ressel family had to come up with $6000 per month to pay for her treatment all by themselves. The high cost of antineoplaston treatment is directly due to the United States government’s refusal to allow any tax-payer money to be granted to fund the FDA-supervised clinical trials that Jessica participated in—while simultaneously granting PhRMA tens of millions of dollars to fund similar FDA-supervised clinical trials with inferior outcomes.
Below is a TV news footage montage from 1996-1997 covering Jessica’s story, fundraisers and more:
The Ronald McDonald House Charities®
During our interview with the Ressel family, Robin said that she “had called the Ronald McDonald House to see if we’d be able to stay there, because we were going to have to stay in Houston for a while, I was talking to a volunteer on the phone—when I mentioned we had an eleven-year old we were taking to see Dr. Burzynski and we needed a place to stay for a couple of weeks—you could hear whispering going on in the background, the volunteer was being prompted what to say, and The Ronald McDonald House refused to allow us to stay there because we weren’t an M.D. Anderson patient. I felt bad for the volunteer, you could tell she was being told what to say.” Dan followed up by saying “There are a lot of programs out there, but I will never give a dime to the Ronald McDonald House. We were in a desperate situation, and they refused us because we were a patient of Dr. Burzynski”.
Joining the Fight in Preserving Burzynski’s Freedom
Jessica Ressel was being treated by Dr. Burzynski in 1996, several months after the FDA’s 5th grand jury against Dr. Burzynski resulted in an indictment. “The government was more frustrating than the cancer itself.” The Ressel family traveled to Washington DC to meet hundreds of other Burzynski patients to speak out against the FDA’s attempt to remove him from society.
Jessica Ressel’s medical records are published by written authorization by Jessica Ressel-Doeden.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}